HL-60-Luc: Non-Invasive Bioluminescence Imaging for Serial Monitoring of Leukemia Treatment Response
Introduction
Acute myeloid leukemia (AML) remains one of the most challenging hematologic malignancies to treat. Although chemotherapy induces remission in the majority of adult patients, relapse occurs in most cases, ultimately leading to fatal outcomes. A critical factor underlying disease relapse is the persistence of small populations of residual leukemic cells that reside within specialized perivascular niches in organs such as the bone marrow, spleen, and liver—sanctuaries that protect these cells from conventional cytotoxic agents.
A landmark 2012 study from Memorial Sloan Kettering Cancer Center (MSKCC), published in Leukemia, leveraged HL-60-Luc cells—human promyelocytic leukemia cells dual-transduced with firefly luciferase and GFP reporters—to demonstrate the power of bioluminescence imaging (BLI) for serial, non-invasive monitoring of systemic leukemia progression and treatment response in vivo. Using the novel vascular disrupting agent (VDA) combretastatin-A1-diphosphate (OXi4503), the investigators achieved statistically significant survival benefits and demonstrated that BLI signals serve as highly sensitive biomarkers of leukemic tumor burden across multiple organ systems.
The HL-60-Luc cell line, derived from the well-characterized HL-60 human promyelocytic leukemia line (ATCC CCL-240), stably expresses firefly luciferase, enabling sensitive detection of as few as 10⁴ cells by BLI. The dual-reporter approach (luciferase for in vivo imaging, GFP for ex vivo tissue validation) makes this cell line uniquely suited for comprehensive preclinical drug evaluation in systemic leukemia models—an application where traditional caliper-based measurements are fundamentally impossible.
Advance your leukemia research with our validated HL-60-Luc cell line. Stable luciferase expression and proven in vivo performance make it ideal for systemic disease modeling and drug screening.
Order Now: HL-60 Cell Line | HL-60-Luc Cell Line
Establishing the Systemic Leukemia Model
The investigators established a rigorous systemic leukemia model by intravenously injecting 1.0 × 10⁷ luc+/GFP+ HL-60 cells into sublethally irradiated SCID/Beige mice. This approach recapitulates the natural hematogenous dissemination pattern of human leukemia, in contrast to subcutaneous xenograft models that fail to capture the systemic nature of the disease. Lentiviral transduction achieved approximately 99% GFP positivity with no alteration in cell viability, proliferative capacity, or morphology compared to non-transduced parental HL-60 cells.
In vitro characterization demonstrated a strong linear correlation (R = 0.993) between BLI flux and cell number across serial dilutions (10⁴ to 5 × 10⁵ cells), confirming the quantitative fidelity of the reporter system. The percentage of GFP-expressing cells correlated strongly with total BLI flux (R = 0.93), establishing that the dual-reporter system provides internally consistent in vivo and ex vivo readouts for tracking leukemic burden.
Following systemic injection, BLI signal initially appeared in the lungs at 5 hours post-inoculation (7.3 × 10⁴ p/s), followed by dramatic increases throughout the body over days 6–13, with particular enrichment in the femur, spine, liver, and lung regions. Whole-body BLI flux ranged from 6.8 × 10⁵ to 2.3 × 10⁸ p/s (ventral) and 4.6 × 10⁵ to 1.4 × 10⁸ p/s (dorsal), illustrating the extensive multi-organ dissemination characteristic of advanced systemic leukemia.
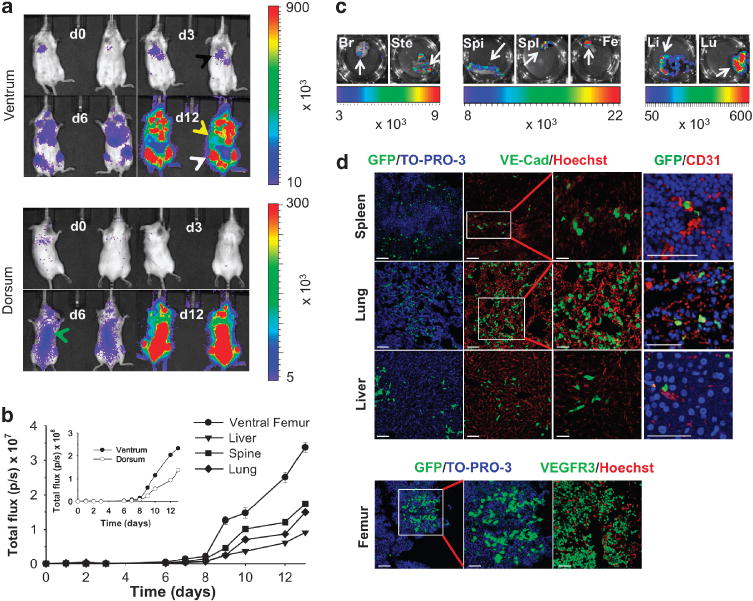
Figure 1. Serial BLI monitoring of systemic leukemic cell migration in SCID/Beige mice. (a) Representative in vivo ventral and dorsal BLI images at days 3, 6, and 12 post-inoculation showing progressive signal accumulation in lung, liver, femur, and spine. (b) Time-series BLI flux for individual organs. (c) Ex vivo BLI of harvested tissues confirming multi-organ engraftment. (d) Immunofluorescence co-localization of GFP+ HL-60 cells with VE-cadherin- and CD31-expressing endothelial cells in spleen, lung, liver, and femur.
Therapeutic Efficacy: OXi4503 in Xenograft Models
Before proceeding to systemic treatment studies, the team first validated the therapeutic efficacy of OXi4503 in a conventional subcutaneous HL-60 xenograft model. Mice bearing hindlimb tumors (78–156 mm³) were treated with OXi4503 (75 mg/kg), the first-generation VDA combretastatin-A4-phosphate (CA4P, 75 mg/kg), the standard chemotherapeutic cytarabine (Ara-C, 20 mg/kg), or saline vehicle. OXi4503 demonstrated dramatically superior tumor control, with essentially constant tumor volumes observed over the treatment interval compared to exponential growth in all other groups (P < 0.001).
At day 23 post-treatment, OXi4503-treated tumors were at least 200-fold smaller than controls. Body weights remained stable throughout treatment, indicating minimal systemic toxicity. Survival analysis confirmed a statistically significant survival benefit for OXi4503-treated mice relative to all other monotherapy arms (P < 0.001). Dose-response evaluation across OXi4503 concentrations (2.5–75 mg/kg/injection) revealed significant tumor growth delays at doses of 10 mg/kg and above, with corresponding improvements in survival at all doses except 2.5 mg/kg.
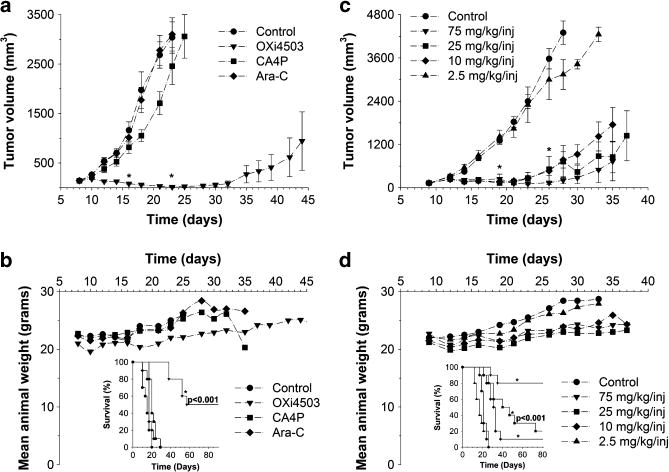
Figure 2. Therapeutic efficacy of OXi4503 in HL-60 xenografts. (a) Time-dependent tumor volume changes after OXi4503, CA4P, Ara-C, or saline treatment. OXi4503 achieved >200-fold tumor reduction vs. controls (*P < 0.001). (b) Stable animal weights and significant survival advantage with OXi4503. (c) Dose-dependent tumor growth delay across OXi4503 concentrations (2.5–75 mg/kg). (d) Corresponding weight profiles and survival data confirming efficacy at ≥10 mg/kg.
Our HL-60-Luc cells provide the quantitative sensitivity needed for rigorous preclinical drug evaluation. Whether testing novel chemotherapeutics, vascular targeting agents, or immunotherapies, HL-60-Luc delivers reliable, real-time in vivo readouts.
Order Now: HL-60 Cell Line | HL-60-Luc Cell Line
Serial BLI Monitoring of Treatment Response in Systemic Models
The pivotal experiment applied OXi4503 (25 mg/kg) treatment to the systemic leukemia model, using BLI to serially monitor therapeutic response in individual mice. Two doses were administered on days 7 and 10 post-inoculation, with BLI imaging performed every 1–3 days. The results were striking: up to a 10-fold reduction in BLI signal was observed across the femur, lung, liver, and spine regions in treated mice compared to untreated controls.
Statistically significant differences in BLI flux between treated (n = 8) and untreated (n = 6) cohorts were confirmed at day 13 for all analyzed tissues (P ≤ 0.001): liver/bowel (P = 0.0015), lung (P = 0.001), ventral femur (P = 0.0005), and spine (P = 0.0005). Importantly, greater signal reductions were observed after the initial dose compared to the second dose for the femur, spine, and lung, suggesting that the first treatment produced the most substantial anti-vascular and cytotoxic effect. The ability to track individual animal responses over time—without sacrificing cohorts at arbitrary endpoints—represents a fundamental advantage of the HL-60-Luc BLI approach.
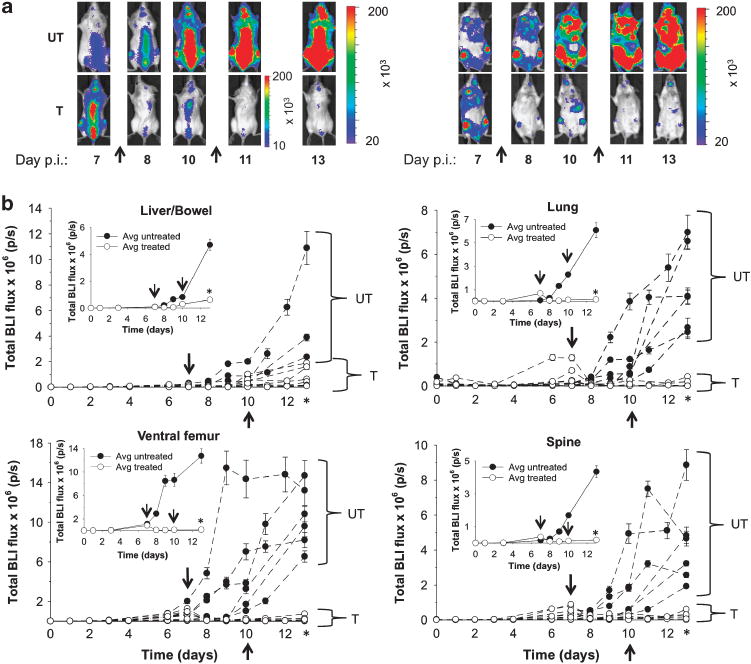
Figure 3. In vivo response monitoring in systemic HL-60 models using BLI. (a) Representative ventral and dorsal BLI images before and after OXi4503 treatment showing progressive signal reduction. Arrows indicate treatment times. (b) Individual animal BLI flux time-courses for liver, lung, femur, and spine, demonstrating significantly greater signal reductions in treated vs. untreated mice (P ≤ 0.001 at day 13).
BLI-Tissue Correlation and Perivascular Niche Discovery
A critical validation step correlated in vivo BLI signals with ex vivo GFP expression levels in harvested tissues. The percentage of GFP+ HL-60 cells was quantified by immunohistochemistry across all major organs. Statistically significant reductions in GFP+ cell populations were confirmed in treated versus untreated tissues, with the greatest differences observed in lung (P = 0.014) and femur (P = 0.014). Strong correlations between BLI flux and % GFP+ expression were demonstrated for treated liver (R² = 0.973), lung (R² = 0.950), femur (R² = 0.861), and spine (R² = 0.929).
Perhaps the most biologically significant finding was the consistent co-localization of GFP+ HL-60 cells with VE-cadherin- and CD31-expressing endothelial cells in all evaluated tissues—both before and after OXi4503 treatment. In the liver, GFP+ cells resided adjacent to VE-cadherin+ endothelial cells. In the femur, similar perivascular localization was observed. Even after treatment, when overall cell numbers were dramatically reduced, surviving GFP+ cells maintained their proximity to vascular endothelium. This finding strongly implicates the perivascular niche as a critical sanctuary for leukemic cell survival and resistance to vascular disrupting therapy, providing a mechanistic explanation for leukemia relapse after treatment.
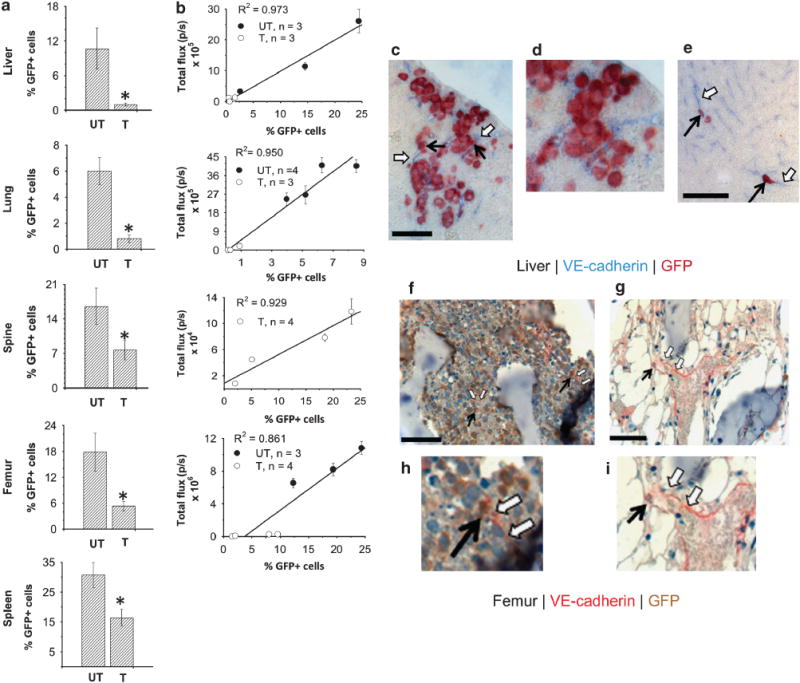
Figure 4. Quantitative GFP expression analysis and perivascular niche co-localization. (a) Tissue-specific % GFP+ cells in treated vs. untreated mice showing significant reductions in lung and femur (P = 0.014). (b) Strong correlation between in vivo BLI flux and ex vivo % GFP+ expression across all tissues. (c–i) Co-labeling of GFP+ HL-60 cells (brown/red arrows) with VE-cadherin+ endothelial cells (blue/open arrows) in untreated and treated liver and femur sections, demonstrating persistent perivascular niche localization after therapy.
Discussion
This study from MSKCC established a powerful paradigm for preclinical leukemia drug evaluation using HL-60-Luc reporter cells and serial BLI monitoring. The key innovations include: (1) a systemic leukemia model that faithfully recapitulates the multi-organ dissemination pattern of human disease; (2) dual-reporter validation (BLI in vivo + GFP ex vivo) ensuring quantitative accuracy; and (3) the demonstration that BLI signal can serve as an exquisitely sensitive biomarker of tumor burden in systemic models, with strong tissue-level correlations (R² up to 0.973).
The therapeutic findings with OXi4503 extend previous work with first-generation VDAs by providing much shorter-term (days-to-weeks rather than months) and more granular treatment response data. The observation that surviving leukemic cells persist within perivascular niches—even after effective vascular disruption—has direct implications for combination therapy design: agents that disrupt protective niche interactions may be necessary alongside VDAs to achieve complete disease eradication and prevent relapse.
For the preclinical research community, this work underscores the unique value of HL-60-Luc as a research tool. Its dual-reporter design supports both real-time in vivo monitoring and rigorous ex vivo validation, its systemic disease model captures clinically relevant multi-organ pathology, and its well-characterized BLI dynamics permit efficient drug screening with dramatically reduced animal numbers compared to endpoint-only study designs.
Conclusion
The HL-60-Luc cell line represents an indispensable tool for systemic leukemia research and preclinical drug discovery. By combining dual luciferase/GFP reporters with bioluminescence imaging, researchers can achieve sensitive, non-invasive, and quantitative monitoring of leukemic cell homing, expansion, and therapeutic response across multiple organ systems in real time. The Benezra et al. study provides a methodological blueprint for leveraging this cell line to evaluate novel therapeutic agents—including vascular disrupting agents, chemotherapeutics, and targeted therapies—with unprecedented temporal resolution and statistical rigor.
Reliable in vivo tumor models are the foundation of impactful preclinical leukemia research. Our HL-60-Luc cell line offers stable luciferase expression, high signal-to-noise ratio, and proven performance in both systemic and xenograft models.
Order Now: HL-60 Cell Line | HL-60-Luc Cell Line
References
Benezra M, Phillips E, Tilki D, et al. Serial monitoring of human systemic and xenograft models of leukemia using a novel vascular disrupting agent. Leukemia. 2012;26(8):1771–1778. doi:10.1038/leu.2012.48
